O Leukoplakia
O Hairy leukoplakia
O Lichen planus
O Lichenoid reactions
O Linea alba
O Nicotinic stomatitis
O Uremic stomatitis
O Cinnamon contact stomatitis
O Chemical burn
O Candidiasis
O Chronic biting
O Geographic tongue
O Hairy tongue
O Furred tongue
O Materia alba of the gingiva
O Fordyce’s granules
O Leukoedema
O White sponge nevus
O Dyskeratosis congenita
O Pachyonychia congenita
O Focal palmoplantar and oral mucosa hyperkeratosis syndrome
O Papilloma
O Verrucous carcinoma
O Squamous-cell carcinoma
O Skin and mucosal grafts
O Epithelial peeling
 |
| White Lesions |
Leukoplakia
Definition Leukoplakia is a clinical term, and the lesion isdefined as a white patch or plaque, firmlyattached to the oral mucosa, that cannot be classified as any other diseaseentity. It is a precancerous lesion.
Etiology The exact etiology remains unknown. Tobacco,alcohol, chronic local friction, and Candida albicansare important predisposing factors. Human papilloma virus (HPV) may also beinvolved in the pathogenesis of oralleukoplakia.
Clinical features Three clinical varieties (Figs. 1 and 2)are recognized: homogeneous (common), speckled(less common), and verrucous (rare). Speckled and verrucous leukoplakia have agreater risk for malignant transformationthan the homogeneous form. The average percentage of malignant transformationfor leukoplakia varies between 4% and 6%. The buccal mucosa, tongue, floor ofthe mouth, gingiva, and lower lip are the most commonly affected sites.
Laboratory tests Histopathological examination.
Differential diagnosis Lichen planus, cinnamon contactstomatitis, candidiasis, hairy leukoplakia,lichen planus reactions, chronic biting, tobacco pouch keratosis, leukoedema,chemical burn, uremic stomatitis, skin graft, some genodermatoses and discoidlupus erythematosus.
Treatment Elimination or discontinuation of predisposingfactors, systemic retinoid compounds.Surgical excision is the treatment of choice.
 |
| Homogeneous leukoplakia. |
 |
| Speckled leukoplakia |
Hairy Leukoplakia
Definition Hairy leukoplakia is one of the most common andcharacteristic lesions of humanimmunodeficiency virus (HIV) infection. Rarely, it can also appear inimmunosuppressed patients after organ transplantation.
Etiology Epstein–Barr virus seems to play an important role inthe pathogenesis.
Clinical features Hairy leukoplakia presents as a whiteasymptomatic, often elevated and unremovable patch. The lesion is almost alwaysfound bilaterally on the lateral margins of the tongue, and may spread to thedorsumand the ventral surface. Characteristically, the surface of thelesion is corrugated with a vertical orientation. However, smooth and flatlesions may also be seen. The lesion is not precancerous.
Laboratory tests Histological examination, in situhybridization, polymerase chain reaction (PCR) and electron microscopy.
Differential diagnosis Chronic biting, lichen planus,frictional keratosis, cinnamon contact stomatitis, uremic stomatitis, candidiasis.
Treatment Not required; however, in some cases acicloviror valaciclovir can be used with success.
 |
| Hairy leukoplakia. |
Lichen Planus
Definition Lichen planus is a relatively common chronicinflammatory disease of the oral mucosa and skin.
Etiology Although the cause is not well known, Tcell-mediated autoimmune phenomena are involved in the pathogenesis of lichenplanus.
Clinical features White papules that usually coalesce, forming anetwork of lines (Wickman’s striae), are the characteristic oral lesionsof the disease. Six forms of the disease are recognized in the oral mucosa, classifiedaccording to frequency: the common ;the less common ; and the rare .Middle-aged individuals are more com-monly affected (the ratio of women to menratio is 3 : 2). The buccal mucosa, tongue, and gingiva are the sites ofpredilection. The skin lesions characteristically appear as polygonal purple,pruritic papules, usually affecting the flexor surfaces of the extremities. Theglans penis and nails may also be affected. The disease can usually bediagnosed on clinical grounds alone. The prognosis of lichen planus is usuallygood, and malignant transformation (particularly of the erosive form) remains controversial.
Laboratory tests Histopathological examination is very helpful.Direct immunofluorescence can also be used, although the features are not specific.
Differential diagnosis Discoid lupus erythematosus, candidiasis, graft-versus-hostdisease, geographic tongue, leukoplakia, erythroplakia, cicatricial pemphigoid,pemphigus, bullous pemphigoid.
Treatment No treatment is needed in asymptomatic lesions.Topical steroids (ointment in Orabase, intralesional injection), may behelpful. Systemic steroids in low doses can be used in severe and extensivecases. The topical use of antiseptic mouthwashes should be avoided.
 |
| Lichen planus of the buccal mucosa: reticular form. |
 |
| Lichen planus of the dorsum of the tongue: hypertrophic form. |
 |
| Lichen planus, papular and reticular forms, of the buccal mucosa |
 |
| Lichen planus, pigmented form, of the buccal mucosa |
Lichenoid Reactions
Definition Lichenoid or lichen planus reactions are aheterogeneous group of lesions of the oral mucosa that show clinical andhistopathological similarities to lichen planus, but have a different course.
Etiology Hypersensitivityto dental restorative materials, amalgam, composite resins and dental plaqueaccumulation are the most common causative factors. Rarely, a reaction to drugsmay be responsible.
Clinical features Clinically, they appear as white and/orerythematous lesions, usually associated with peripheral delicate white striae.
Erosions are alsocommon . The lesions mimic erosive lichen planus. Characteristically, thelesions are strictly confined to the mucosa directly in contact with therestorative materials, and do not migrate to other sites. The lesions disappearafter removal of the adjacent material.
The diagnosis isusually made clinically.
Laboratory tests Askin punch test may be helpful in some cases.
Differential diagnosis Lichen planus, fixed drug eruption, discoidlupus erythematosus, cicatricial pemphigoid, cinnamon contact stomatitis.
Treatment Replacementof the restorative material, polishing and smoothing, and good oral hygiene arerecommended. Topical steroid treatment for a short time is also helpful.
 |
| Lichanoid drug reaction to allopurinol: white hyperkeratotic lesions and superficial erosions on the sides of the tongue. |
 |
| Lichenoid reaction to dental amalgam and cold: white and erythematous lesions on the buccal mucosa |
Linea Alba
Definition Linea albais a relatively common alteration of the buccal mucosa.
Etiology Pressure,sucking fromthe buccal surface of the teeth.
Clinical features It presents as an asymptomatic, bilateral,linear elevation with a slightly whitish color at the level of the occlusalline of the teeth. It has a normal consistency on palpation. The diagnosis isbased on clinical grounds alone.
Treatment No treatmentis required.
 |
| Linea alba. |
Nicotinic Stomatitis
Definition Nicotinicstomatitis, or smoker’s palate, is a common tobacco- related type ofkeratosis that occurs exclusively on the hard palate, and is classicallyassociated with heavy pipe and cigar smoking.
Etiology The elevated temperature, rather than thetobacco chemicals, is responsible for this lesion.
Clinical features Clinically,the palatal mucosa initially responds to the high temperature with redness.Later, it becomes wrinkled and takes on a diffusely grayish-white color, withnumerous micronodules with characteristic punctate red centers, which representthe inflamed and dilated orifices of the minor salivary gland ducts. Thelesions are not premalignant, in contrast to the “reverse smoker’s palate” lesion,which is associated with reverse smoking.
Laboratory tests Usually not required. However, ahistopathological examination is useful.
Differential diagnosis Reverse smoker’s palate, leukoplakia,discoid lupus erythematosus, candidiasis, lichen planus.
Treatment Cessation ofsmoking.
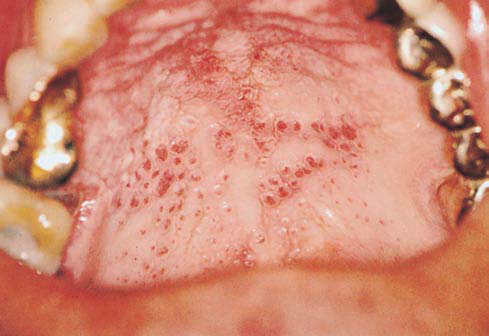 |
| Nicotinic Stomatitis |
Uremic Stomatitis
Definition Uremicstomatitis is a rare disorder that may occur in patients with acute or chronicrenal failure.
Etiology Increasedconcentration of urea and its products in the blood and saliva. Thepathogenesis of oral lesions is not clear. It usually appears when bloodconcentration of urea exceeds 30 mmol/1. The degradation of oral urea by theenzyme urease forms free ammonia, which may damage the oral mucosa.
Clinical features Four forms of uremic stomatitis are recognized:(a) the ulcerative form, (b) the hemorrhagicform, (c) the nonulcerative, pseudomembranous form, and (d) the hyperkeratotic form. The last two forms appear as white lesions. The nonulcerative,pseudomembranous form presents as painful diffuse erythema covered by a thickwhitish-gray pseudomembrane. The hyperkeratotic formpresents asmultiple painfulwhite hyperkeratotic lesions with thin projections. The tongue, and the floorof the mouth are more frequently affected. Xerostomia, uriniferous breath odor,unpleasant taste, and a burning sensation are common symptoms. Candidiasis andviral and bacterial infections are common oral complications. The diagnosis isbased on the history, the clinical features, urinalysis and blood urea leveldetermination.
Differential diagnosis Candidiasis, cinnamon contactstomatitis, hairy leukoplakia, white sponge nevus, drug reactions.
Treatment The orallesions usually improve after hemodialysis. A high level of oral hygiene,mouthwashes with oxygen release agents, and artificial saliva are suggested.Antimycotic, antiviral, and antimicrobial agents if necessary.
 |
| Uremic stomatitis, white hyperkeratotic lesions mimic hairy leukoplakia on the lateral border of the tongue |
 |
| Uremic stomatitis, whitish-gray pseudomembranes on the tongue and floor of the mouth. |
Cinnamon ContactStomatitis
Definition Cinnamoncontact stomatitis is a relatively common oral mucosal reaction to continuouscontact of substances with cinnamon.
Etiology Artificialcinnamon flavoring especially in the form of chewing gum, candies, toothpaste,drops, etc.
Clinical features The condition is characterized by erythema ofthe oral mucosa, usually in association with desquamation and erosions. Whitehyperkeratotic plaques are very common. A burning sensation and pain are commonsymptoms. The lateral borders of the tongue, the buccal mucosa, and the gingivaare more frequently affected. Exfoliative cheilitis and perioral dermatitis mayoccur. The diagnosis is based on the history and the clinical features.
Differential diagnosis Amalgam contact stomatitis, chronic biting, leukoedema,epithelial peeling, hairy leukoplakia, leukoplakia, candidiasis, uremicstomatitis, lichen planus, discoid lupus erythematosus.
Treatment Discontinuationof any cinnamon product improves the signs and symptoms in approximately twoweeks. In severe and extended lesions with erosions, low doses of steroids(e.g., 10 mg/day prednisolone) for one week help the lesions to heal.
 |
| Cinnamon ContactStomatitis |
 |
| Cinnamon ContactStomatitis |
Chemical Burn
Definition This is aninjury to the oral mucosa caused by topical application of caustic agents.
Etiology Causative agents include aspirin, hydrogenperoxide, phenol, alcohol, sodiumperb orate, silver nitrate, trichloroaceticacid, acid etching liquid, and varnishes of tooth cavities.
Clinical features Clinically, the affected mucosa is covered with a white membrane due to necrosis.The necrotic epitheliumcan easily be scraped off, leaving a red, bleedingsurface. The lesions are painful. The diagnosis should be made on the basis ofthe clinical features and history.
Differential diagnosis Necrotizing ulcerative gingivitis andstomatitis, materia alba, candidiasis, mechanical trauma, bullous diseases.
Treatment Treatment issymptomatic.
 |
| Aspirin Burn |
 |
| Phenol burn |
 |
| Trichloroaceticacid burn |
Candidiasis
Definition Candidiasisis the most common oral fungal infection. Over the last two decades, thedisease has taken on major importance.
Etiology It is usually caused by Candida albicans, and less frequently by other fungal species (C. glabrata, C. krusei, C. tropicalis, C. parapsilosis). Predisposing factors are local (poor oral hygiene, xerostomia,mucosal damage, dentures, antibiotic mouthwashes) and systemic (broad-spectrum antibiotics,steroids, immunosuppressive drugs, radiation, HIV infection, hematologicalmalignancies, neutropenia, iron-deficiency anemia, cellular immunodeficiency,endocrine disorders).
Clinical features Oral candidiasis is classified as primary, consisting of lesions exclusively on the oraland perioral area, and secondary,consisting of oral lesions of mucocutaneous disease. Primary candidiasisincludes five clinical varieties: pseudomembranous, erythematous, nodular, papillaryhyperplasia of the palate, and Candida-associated lesions (angular cheilitis, median rhomboid glossitis,denture stomatitis). The main forms of candidiasis that produce white lesionsare the following.
Pseudomembranous candidiasis is the most common form of the disease, and is clinically characterized bycreamy-white, slightly elevated, removable spots or plaques. The lesions may belocalized or generalized, and appear more frequently on the buccal mucosa, softpalate, tongue, and lips. Xerostomia, a burning sensation, and an unpleasant tasteare the most common symptoms.
 |
| Pseudomembranous candidiasis |
 | |||||||
| Nodular candidiasis |
 |
| Nodular candidiasis |
Nodular candidiasis is a chronic formof the disease; it appears clinically as a white,firm, and raised plaque that usually does not detach.
Mucocutaneous candidiasis is a heterogeneous and rare group of clinical syndromes, characterized bychronic lesions of the skin, nails, and mucosae, and usually associated withimmunological defects. Clinically, the oral lesions appear as white and usuallymultiple plaques, which cannot be removed.
Laboratory tests Cytology and tissue culture examination; biopsyonly in chronic cases.
Differential diagnosis Leukoplakia, hairy leukoplakia, lichen planus, syphiliticmucous
patches, white sponge nevus, chemical and traumatic lesions, cinnamoncontact stomatitis, lupus erythematosus.
Treatment Topicalantifungal agents (nystatin, azole derivatives, amphotericin B). Systemicazoles (ketoconazole, fluconazole, itraconazole).
Chronic Biting
Definition and etiology Mild chronic biting of the oral mucosa is relatively common in nervousindividuals. These patients consciously bite the buccal mucosa, lips, and tongue,and detach the superficial epithelial layers.
Clinical features The lesions are characterized by a diffuseirregular white area of small furrows and desquamation of the epithelium.Rarely, erosions and petechiae may be seen. The diagnosis is made clinically.
Differential diagnosis Candidiasis, lichen planus, leukoplakia, hairy leukoplakia, white sponge nevus,leukoedema, cinnamon contact stomatitis.
Treatment Recommendation to stop the habit.
 |
| Cheek Biting |
Geographic Tongue
Definition Geographictongue, or erythema migrans, is a relatively common benign condition, primarilyaffecting the tongue and rarely other oral mucosa sites (geographicstomatitis)
Etiology The exactetiology remains unknown. It may be genetic.
Clinical features Clinically, the condition is characterized bymultiple, well-demarcated, erythematous, depapillated patches, typicallysurrounded by a slightly elevated whitish border, and usually restricted to thedorsumof the tongue. Characteristically, the lesions persist for a short timein one area, then disappear completely and reappear in another area. Thecondition is usually asymptomatic, and often coexists with fissured tongue. Thediagnosis is made clinically.
Differential diagnosis Candidiasis, lichen planus, psoriasis, Reitersyndrome,
syphilitic mucouspatches.
Treatment Reassuranceof the patient.
 |
| Geographic tongue |
 |
| Geographic tongue-Localized lesion |
 |
| Geographic tongue with prominent whitish border |
Hairy Tongue
Definition Hairytongue is a relatively common disorder that is due to marked accumulation ofkeratin on the filiform papillae of the tongue, resulting in a hairlikepattern.
Etiology Unknown.Predisposing factors are poor oral hygiene, oxidizing mouthwashes, antibiotics,excessive smoking, radiation therapy, emotional stress, and bacterial and Candidaspecies infections.
Clinical features Clinically, it is characterized by anasymptomatic elongation of the filiformpapillae of the dorsum of the tongue,sometimes extending over several millimeters. The color may range from whitishto brown or black. The diagnosis is made clinically.
Treatment Eliminationof predisposing factors, brushing of the tongue,local use of keratolytic agents(trichloroacetic acid, podophyllin).
 |
| Hairytongue |
 |
| Hairytongue |
 |
| Hairytongue |
Furred Tongue
Definition Furredtongue is a relatively uncommon disorder, usually appearing during febrileillnesses.
Etiology The cause isnot clear. Predisposing factors are febrile painful oral lesions, poor oralhygiene, dehydration, and soft diet.
Clinical features Clinically, it appears as a white orwhitish-yellow thick coating on the dorsal surface of the tongue . The lesionis due to lengthening of the filiformpapillae, by up to 3–4 mm,and accumulation of debris and bacteria. Characteristically, furred tongue appearsand disappears within a short period. The diagnosis is made clinically.
Differential diagnosis Hairy tongue, hairy leukoplakia, candidiasis.
Treatment Therapy ofthe underlying illnesses and improvement of oral hygiene.
 |
| Furredtongue |
Materia Alba of theGingiva
Definition and etiology Materia alba results fromthe accumulation of fooddebris, dead epithelial cells, and bacteria. It is common at the dentogingivalmargin. Rarely, materia alba may be seen along the vestibular surface of theattached gingiva in patients with poor oral hygiene.
Clinical features It presents as a soft, whitish plaque that iseasily detached after slight pressure.
Differential diagnosis Candidiasis, chemical burn, leukoplakia.
Treatment Good oralhygiene
 |
| White plaques on the attached gingiva and the alveolar mucosa, caused by materia alba accumulation |
Fordyce’sGranules
Definition Fordyce’sgranules are ectopic sebaceous glands of the oral mucosa.
Etiology It is anormal anatomical variation.
Clinical features Clinically, the granules present as multiple,asymptomatic, slightly raised whitish-yellow spots. The vermilion border of theupper lip, the commissures, and the buccal mucosa are the sites ofpredilection. They occur in about 80% of adults of both sexes. The diagnosis isbased on the clinical features alone.
Differential diagnosis Lichen planus, leukoplakia, candidiasis.
Treatment No treatmentis required.
 |
| Fordyce’sgranules |
Leukoedema
Definition Leukoedema is a normal anatomical variation.
Etiology It is due to increased thickness of theepitheliumand intracellular edema of the prickle-cell layer.
Clinical features Clinically, it is characterized by a grayish-white, opalescent pattern of themucosa and a slightly wrinkled surface, which characteristically disappearswhen the mucosa is everted and stretched. It usually occurs bilaterally on thebuccal mucosa, and rarely on the tongue and lips.
Differential diagnosis Leukoplakia, hairy leukoplakia, lichen planus.
Treatment No treatment is required.
 |
| Leukoedema of the buccal mucosa. |
White Sponge Nevus
Definition Whitesponge nevus, or Cannon disease, is a relatively rare genodermatosis.
Etiology Genetic. Itis inherited as an autosomal dominant trait.
Clinical features It presents as symmetrical white lesions withmultiple furrows and a spongy texture. The lesions may appear at birth, or morecommonly in early childhood. The buccal mucosa and the ventral surface of thetongue are the sites of predilection, although lesions may develop anywhere inthe mouth, or even in the vaginal and rectal mucosa.
Laboratory tests Histopathological examination.
Differential diagnosis Leukoedema, leukoplakia, lichen planus, chronicbiting, dyskeratosis congenita, pachyonychia congenita.
Treatment No treatmentis required.
 |
| Whitesponge nevus |
Dyskeratosis Congenita
Definition Dyskeratosiscongenita, or Zinsser–Engman–Cole syndrome, is an uncommon disorder.
Etiology Genetic. Itis probably inherited as a recessive autosomal and X-linkedtrait.
Clinical features It is characterized by hyperpigmentation, atrophicskin areas, telangiectasia, nail dystrophy, hyperhidrosis, skin and mucosal bullae,blepharitis and ectropion, anemia, and oral manifestations. The oral lesionsconsist of recurrent blisters, epithelial atrophy, and leukoplakia.Squamous-cell carcinoma may occur.
Differential diagnosis Leukoplakia, lichen planus, epidermolysisbullosa,
pachyonychia congenita.
Treatment Supportive.
 |
| Dyskeratosiscongenita |
Pachyonychia Congenita
Definition Pachyonychiacongenita, or Jadassohn–Lewandowski syndrome, is an uncommongenodermatosis.
Etiology Genetic. Itis inherited as an autosomal dominant trait.
Clinical features It is characterized by symmetrical nailthickening, palmoplantar hyperkeratosis, hyperhidrosis, blister formation,follicular keratosis, and oral lesions. The oral lesions appear at birth orshortly afterward, and present as thick and white or grayish-white plaques, usuallyon the buccal mucosa, the tongue, and the gingiva. The diagnosis is based onthe history and the clinical features.
Differential diagnosis Dyskeratosis congenita, leukoplakia, lichenplanus, white sponge nevus, and focal palmoplantar and oral mucosahyperkeratosis syndrome.
Treatment Supportive.
 |
| Focal palmoplantar hyperkeratosis |
 |
| Pachyonychia congenita: grayish-white lesion on the buccal mucosa |
Focal Palmoplantar andOral Mucosa Hyperkeratosis Syndrome
Definition This is arare mucocutaneous disorder.
Etiology Genetic. Itis inherited as an autosomal dominant trait.
Clinical features The main clinical manifestations are focalhyperkeratosis on the weight-bearing and pressure-related regions of the palms,soles, and oral mucosa. Rarely, thickening of the nails and hyperhidrosis maybe seen. The oral lesions present as white hyperkeratotic plaques(leukoplakia), mainly on the attached gingiva, the lateral border of thetongue, and the palate. The lesions usually develop in early childhood.
Differential diagnosis Pachyonychia congenita, dyskeratosis congenita,leukoplakia.
Treatment Supportive.Retinoids may be helpful.
 |
| Focal Palmoplantar andOral Mucosa Hyperkeratosis Syndrome |
Papilloma
Papilloma appears asan exophytic, painless, usually pedunculated growth. Characteristically, thetumor has a white or normal color, with numerous fingerlike projections thatform a cauliflower pattern. Papilloma is usually solitary, with a size of 0.5–1 cm.
 |
| Papilloma on Buccal Mucosa |
Verrucous Carcinoma
Definition Verrucouscarcinoma is a low-grade variant of squamouscell
carcinoma.
Etiology Human papillomavirus is presumably involved inthe pathogenesis.
Clinical features Clinically, it presents as an exophytic whitemass with a verrucous or pebbly surface. The size varies from1 cm in the earlystages to very extensive lesions. The buccal mucosa, palate, and alveolarmucosa are the most common sites of involvement. Verrucous carcinoma mainlydevelops in smokers over 60 years of age.
Laboratory tests Histopathological examination.
Differential diagnosis Verrucous leukoplakia, papilloma, verruciform xanthoma,white sponge nevus, squamous-cell carcinoma.
Treatment Surgical excision.
 |
| Verrucous Carcinoma |
Squamous-CellCarcinoma
Squamous-cellcarcinoma has a wide spectrum of clinical features. In about 5–8% ofcases, it appears in the early stages as a white asymptomatic plaque identicalto leukoplakia. Biopsy and histopathological examination areimportant for the diagnosis in these cases.


Skin and MucosalGrafts
Definition Skin and mucosalgrafts are often utilized in the oral cavity to cover mucosal defects afterextensive surgery for benign and malignant tumors, or as free gingival graft.
Clinical features clinically, both forms of grafts (skin andmucosal) usually present as a whitish, or gray-white plaque. The size of theplaque depends on the size of the graft. Occasionally, the color of the skingraft is black, due to melanin overproduction. If the graft contain hairfollicles, hairs may develop in the oral cavity. The tongue, buccal mucosa,palate, gingiva and alveolar mucosa are the most common sites where skin andmucosal grafts are placed. Skin graft into the oral cavity may be associatedwith unpleasant feelings. The diagnosis is based on the history and theclinical features.
Differential diagnosis Leukoplakia, traumatic scar, epidermolysisbullosa.
Treatment No treatmentis required.
 |
| Skin and mucosalgrafts |
 |
| Skin and mucosalgrafts |
Epithelial Peeling
Definition Epithelialpeeling is a relatively common superficial desquamation
(epitheliolysis) of theoral mucosa.
Etiology It is causedby the direct irritating effect of toothpastes that contain sodium laurylsulfate or pyrophosphates. The same phenomenon may be associated withchlorhexidine mouthwash. Sometimes the lesions are idiopathic.
Clinical features Clinically, epithelial peeling presents assuperficial painless white plaques or dots that can be easily lifted fromtheoral mucosa. The buccal mucosa, lip mucosa, and mucobuccal and mucolabial foldsare more frequently affected. The lesions usually disappear when the individualstops using these toothpastes or mouthwashes. The diagnosis is based entirelyon the history and the clinical features.
Differential diagnosis Chemical burn, chronic biting, candidiasis,leukoplakia.
Treatment Discontinuationof responsible toothpastes or mouthwashes.
 |
| Mucosal Peeling |
But Dr. Itua, Traditional Herbal Practitioner in Africa, has cured HIV which is extracted from some rare herbs. It is highly potential to cure AIDS 100% without any residue. Dr Itua herbal medicine has already passed various blogs on how he uses his powerful herbs to heal all kinds of diseases such as. Herpes, HIV,,Cushing’s disease,Heart failure,Multiple Sclerosis,Hypertension,Colo_Rectal Cancer, Diabetes, Hepatitis,Hpv,Weak ErectionLyme Disease,Blood Cancer,Alzheimer’s disease,Bechet’s disease,Crohn’s disease,Parkinson's disease,Schizophrenia,Lung Cancer,Breast Cancer,Colo-Rectal Cancer,Blood Cancer,Prostate Cancer,siva.Fatal Familial Insomnia Factor V Leiden Mutation ,Epilepsy Dupuytren's disease,Desmoplastic small-round-cell tumor Diabetes ,Coeliac disease,Creutzfeldt–Jakob disease,Cerebral Amyloid Angiopathy, Ataxia,Arthritis,Amyotrophic Lateral Scoliosis,Fibromyalgia,Fluoroqquinolone Toxicity,Brain Cancer,Breast Cancer,Lung Cancer,Kidney Cancer,Syndrome Fibrodysplasia Ossificans ProgresS sclerosis,Seizures,Alzheimer's disease,Adrenocortical carcinoma.Asthma,Allergic diseases.Hiv_ Aids,Herpe ,Copd,Glaucoma., Cataracts,Macular degeneration,Cardiovascular disease,Lung disease.Enlarged prostate,Osteoporosis.Alzheimer's disease,Dementia.,Wart Remover,Cold Sore, Epilepsy, also his herbal boost immune system as well. I'm telling this because he uses his herbal medicine to cure me from hepatitis B and HIV, which I have been living on for 9 months now with no side effects. Herbal Medicine is just as good when drinking it although i have to use the restroom after drinking it which I don't really care about because i just want to get the virus out of my body, I will recommend Dr Itua to anyone sick out here to contact Dr Itua with this following information.Email...drituaherbalcenter@gmail.com /
ReplyDeleteWhatsapp Or Call...+2348149277967.
He might be late to respond because he is always busy with patents, but he will surely get back to you with a positive response.